- Review
- Open access
- Published:
MRI and CBCT image registration of temporomandibular joint: a systematic review
Journal of Otolaryngology - Head & Neck Surgery volume 45, Article number: 30 (2016)
Abstract
Purpose
The purpose of the present review is to systematically and critically analyze the available literature regarding the importance, applicability, and practicality of (MRI), computerized tomography (CT) or cone-beam CT (CBCT) image registration for TMJ anatomy and assessment.
Data sources
A systematic search of 4 databases; MEDLINE, EMBASE, EBM reviews and Scopus, was conducted by 2 reviewers. An additional manual search of the bibliography was performed.
Inclusion criteria
All articles discussing the magnetic resonance imaging MRI and CT or CBCT image registration for temporomandibular joint (TMJ) visualization or assessment were included.
Results and included articles’ characteristics
Only 3 articles satisfied the inclusion criteria. All included articles were published within the last 7 years. Two articles described MRI to CT multimodality image registration as a complementary tool to visualize TMJ. Both articles used images of one patient only to introduce the complementary concept of MRI-CT fused image. One article assessed the reliability of using MRI-CBCT registration to evaluate the TMJ disc position and osseous pathology for 10 temporomandibular disorder (TMD) patients.
Conclusion
There are very limited studies of MRI-CT/CBCT registration to reach a conclusion regarding its accuracy or clinical use in the temporomandibular joints.
Background
Merging different imaging modalities such as magnetic resonance imaging (MRI), multi-detector computed tomography (CT) and Positron emission tomography (PET) to display both osseous and soft tissues has been undertaken for about 20 years in neurosurgery [1]. Digital registration tools were employed to optimize image alignment. Other medical applications of image registration have been introduced including computer-aided robotic orthopedic surgeries and radiotherapies [2–4].
Image superimposition to evaluate changes in facial soft tissues, skeleton and dentition has been performed for many years using two-dimensional (2D) radiographs [5, 6]. However, the 2D radiographs suffered many limitations such as tissue overlapping, landmark obstruction, distortion, magnification and object displacement. The contribution of three-dimensional (3D) cone-beam CT (CBCT) to the field of dentistry is significant especially for diagnosis, treatment planning of craniofacial structures and assessment of the hard tissues of the temporomandibular joint (TMJ) [7, 8]. CBCT overcame the limitations of 2D radiography and allows 3D image superimposition. CBCT superimposition using anatomical landmarks in the skull base to analyze changes in craniofacial bones and airway tract has been validated [9–11]. Virtual 3D surface models have been developed to quantify tissue displacement between two time points using a color-coded scale [12, 13]. Registration of CBCT images has evolved into automatic superimposition of 2 CBCT images using the mutual information registration concept and has recently been introduced as a new tool to evaluate the craniofacial changes and TMJ assessment [14, 15].
In 1998, Nebbe et al. superimposed sagittal MRI to lateral cephalometric radiographs to evaluate the temporomandibular joint (TMJ) disc position [16]. CBCT and MRI are the most commonly used diagnostic imaging techniques used in the field of dentistry. CBCT is optimum for viewing skeletal and dental tissues, and MRI is the standard for viewing masticatory muscles, ligaments and the cartilagenous disc of TMJ. Unlike registration of serial CBCT images, multimodality image registration between MRI and CBCT is challenging due to differences in voxel size, pixel intensity, anatomical structure identification, image orientation and field of view (FOV). Nevertheless, this registration is desirable as it provides a complementary image of soft and hard tissues in one picture frame for optimum diagnosis, treatment planning, and evaluation of treatment outcome.
The purpose of the present review is to systematically and critically analyze the available literature regarding importance, applicability, and practicality of MRI, CT and CBCT image registration for TMJ anatomy and assessment.
Materials and methods
Search strategy
Systematic search of four major databases, MEDLINE (1946 to 2015 Jan 10), All EBM Reviews-Cochrane DSR, DARE, and American College of Physicians Journal Club (1980 through January 13, 2016), Scopus (1965 through Jan 18, 2016), and EMBASE (1974 to 2016 January 18), [3] was conducted without language limitation. The search’s key words used were Magnetic resonance imaging, tomography, computed tomography, CT, cone-beam CT, registration, integration, merging, correlation, fusion, superimposition, image-processing, matching, temporomandibular joint, TMJ, temporomandibular disorder, TMD, craniomandibular disorder, TMJ articular disc, TMJ articular disk.
MESH keywords and truncated terms were searched with help of a librarian. In addition, manual search of the references in the identified articles was performed to avoid missing relevant articles. Additional file 1 shows the specific combination of the search terminology in different databases.
Inclusion and exclusion criteria
Studies of different designs (e.g., clinical trials, cohort studies, case–control studies, cross-sectional studies, prospective and retrospective studies, case series/reports) reporting MRI and CT/CBCT image registration for TMJ concerns were included. Reviews, editorials, letters, published errata and historical articles were not included. Articles describing multimodal image registration concerning head and neck oncology were excluded.
Screening process and data collection
Three independent reviewers (M.A., H.S & N.A.) screened the search data thoroughly and identified the relevant abstracts for full-text article evaluation. When in doubt or unclear from the abstract, the full-text article was selected for evaluation. Preliminary selected abstracts/articles, were reviewed according to the inclusion/exclusion criteria. No clear conflict in the article selection between the two reviewers was reported. Image characteristics and registration type for the included studies were collected and summarized in Table 1.
Results
Data searched
The database search resulted in a total of 673 articles. The initial review of the titles and abstracts resulted in 61 articles that were considered for full-text review. The full-text review resulted in 6 articles [15, 17–21]. One more article was identified by manual search [22]. Figure 1 demonstrates a flow chart of the articles selection process. Only 3 articles met the inclusion criteria of this review. The 4 remaining articles from the final selection phase were excluded for the following reasons:
-
1.
Measure accuracy of different multimodal image registration techniques [17, 18].
-
2.
Introducing multimodal image registration to visualize the tumors in the head and neck region [20, 21].
Fig. 1 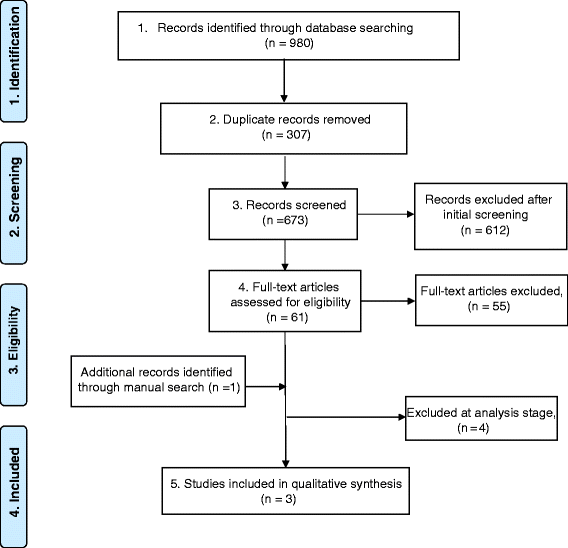
PRISMA 2009 Flow diagram

Characteristics of the included articles
All included articles were published within the last 7 years. Two articles described MRI to CT multimodality image registration as a complementary tool to visualize TMJ. Both articles used images of one patient only to introduce the complementary concept of MRI-CT fused image. One article assessed the reliability of using MRI-CBCT registration to evaluate the TMJ disc position and osseous pathology in 20 TMJ’s for 10 temporomandibular disorder (TMD) patients. Table 1 shows the imaging protocols and measured outcomes of the included articles.
Discussion
Multimodal image registration
The essential goal of merging two images from different modalities is to utilize the complementary nature of the displayed information. Proper registration of the different images is crucial especially when used for clinical applications. The process of image registration is composed of two major steps: the first step is the spatial alignment of the target images, which is commonly defined as “registration, and the second is the fused display of the target images, which is defined as “fusion”. Mistakenly, different terminologies have been inter-changeably used in the literature to describe a single step process: such as superimposition, matching, integration, merging and correlation.
According to van den Elsen et al. and Maintz et al., [23, 24] the registration process was classified into intrinsic and extrinsic models. The intrinsic model depends on anatomical landmarks and segmented bodies or voxel values. The extrinsic model depends on fiducial markers that are either invasively screwed into the tissues or non-invasively attached to the surface skin. Screw-mounted fiducial markers have been considered a gold standard approach for many years to measure the accuracy of the registration process. However, the invasiveness of this approach limits its use to surgical procedures and in-vitro experiments. Anatomical landmarks in the intrinsic registration models are often conspicuous and easy to locate in the human head, however; registration of large tissues in complex regions requires detection of a large number of anatomical landmarks. User interaction is also required to identify the landmarks, which can implicate an operator-bias especially with inexperienced operators. Due to the high degree of similarity between same modality images, monomodal image registration is considered a much easier process than multimodality image registration. In multimodality image registration, such as MRI and CT or CBCT, identifying matched anatomical landmark is a challenging task. Another intrinsic approach is using voxel values (gray values) of the image to spatially align the center of gravity and principal orientation of two images. Using the full image content of gray values in a relative entropy histogram, a method known as “maximization of mutual information”, is a conceptually appealing technique due to its flexibility, easy implementation, automatic and fast use in multimodal image registration (Fig. 2). However, accuracy concerns and sophisticated computational requirements/costs have delayed the clinical application of this registration technique.

Sagittal view of registered PD-weighted MRI (grey color) and CBCT image (Red color) using maximum mutual information algorithm (intrinsic based registration). The inset shows close-up of the TMJ with excellent superimposition of the TMJ anatomical tissues, despite the different receivers, FOV size, voxel size, voxel value, image-acquired orientation, slice thickness, image resolution and field inhomogeneity
For TMJ pathology, MRI or CBCT are the choice of diagnostic imaging depending on availability and the therapeutic indication. Despite the advancement in MR imaging quality, it has not entirely overcome the limitations of the low quality presentation of the complex osseous structure of the TMJ. CBCT is superior at identifying cortical bone contouring, remodeling, developmental abnormality and pathological changes. Both imaging techniques have their limitations and remain complementary to each other in the TMJ diagnostic field.
Accuracy of the MRI-CT/CBCT image registration
Registration technique accuracy is a substantial issue when it comes to multimodality image registration. MRI-CT image registration, using maximum mutual information, have been proven accurate in many medical-imaging related studies [25–28]. The linear measurement error (target error) ranged between 0.4-1.6 mm when registered images in the brain, skull and nasopharynx regions. Three studies have reported the accuracy of registration of MRI to CBCT images [17, 18, 29]. Pawiro et al. used fixed fiducial markers, to a cadaver swine head as a gold standard, to measure the accuracy of mutual information based registration of MRI to C-arm CBCT [17]. The registration target error ranged between 0.62 ± 3.19 mm to 1.5 ± 2.3 mm. Tai et al. used a complicated procedure, which involved multiple steps in five different computational software products, to register large FOV 3D MRI to CBCT image [18]. Although this registration technique was cumbersome and somewhat impractical for clinical use, the authors reported a small target error 0.29-0.71 mm when measured against orthodontic dental models. Al-Saleh et al. used fixed fiducial markers to 5 cadaver swine heads to measure the linear target error of MRI-CBCT image registration [29]. The authors’ findings demonstrated a small linear target error (0.2 ± 1.2 mm) when compared to a laser scanner ground truth value. The accuracy of the multi-modality rigid registration has been proven accurate and accessible in the modern advanced imaging technology.
Review included articles
Lin et al. was the first to explore the 3D rendering of mandible from MRI and CT registered images [22]. One volunteer was scanned in MRI and CT scanner with 12 fiducial markers attached to the facial skin-surface. The centroids of the markers were identified to detect the center of gravity and spatial relation required for rigid registration. It was not clear how the centroids of the spherical markers were detected, or type of images that were utilized to detect the markers centroid. The authors did not describe the type of the surface coil used for MRI or the voxel size difference between the MRI and CT. Moreover, the registration algorithm/ methods, accuracy, or operator’s bias to manually detect the markers’ centroids were not reported. Extrinsic marker-based registration is rapid and conceptually straightforward, but lacks accuracy. Registration target errors, due to marker displacement (especially when attached to skin), patient position and movement, are not possible to control and substantially affect the registration function. The article’s main objective was to draw the readers’ attention to the feasibility of the MRI-CT registration process and its potential in TMJ anatomical screening. However, the report was simple and lacked details of technical and clinical reporting.
In a brief clinical report, Dai et al. [19] highlighted the importance of merging the MRI and CT images to visualize TMJ tissues. The authors chose one sagittal slice of TMJ MRI and CT images from a previous study, as an example, to illustrate a hybrid image of TMJ via Photoshop® software. Since the image processing applied was not a real registration of two images, the authors indicated in their report that the method was not accurate, and it was merely an example of a future endeavor.
Al-Saleh et al. published the first study that employed MRI and CBCT registered images to assess diagnostic reliability of TMJ pathology [15]. Three radiologists evaluated the quality of two techniques of image registration, extrinsic (fiducial marker-based) versus intrinsic (voxel value mutual information based) in 20 TMJ images. The authors reported poor quality and inaccurate extrinsic MRI-CBCT registration when using 5 skin surface attached markers. The poor alignment of the MRI and CBCT images was attributed to the displacement of the markers, and different patient positioning during imaging. Patients were at supine position during MRI and upright position during CBCT imaging. Matching surface markers seems to be insufficient nor reliable. In contrast, the mutual-information based registration was found to be accurate by all radiologists with high intra- and inter-examiner agreement. Moreover, TMJ osseous pathology and articular disc positon were assessed by all radiologists in 3-interval time. The study found that registered MRI-CBCT images have improved the consistency among radiologists in TMJ disc position evaluation. Although that study did not report the actual registration algorithm or the registration linear target error, it highlighted the importance of viewing well-defined osseous contours and articular disc tissue in one image [15]. Fused MRI and CBCT images have better diagnostic value than the value of each image alone. Several challenges in multimodality image registration starting with, but not limited to, the different receivers, FOV, voxel size, voxel value, image-acquired orientation, slice thickness, image resolution, field inhomogeneity and image artifacts, were largely overcome with the recently introduced robust registration model (mutual information). Although mutual information based image registration is a popular technique in medical image processing, it has not yet been explored in the dental field except for two studies, the one by Al-Saleh et al. [15] and another one for monomodality registration (i.e. two CBCT’s) by Choi and Mah [14]. In addition, the study had a small sample size that could have biased the reported results.
Unlike the medical field, studies about the MRI-CT/CBCT image registration are sparse in the field of dentistry. Out of three studies included in this review, [15, 19, 22] only one study utilized the MRI-CBCT image registration for clinical investigation [15]. The need for well-designed studies in this area is clear.
Multimodality MRI-CBCT image registration has potential to meet clinical needs for simultaneous evaluation of soft and hard tissues at complex structures such as the TMJ, in the field of dentistry and craniofacial surgery. However, multimodal image registration technology is relatively young and there is little evidence regarding its clinical use in many areas in dentistry. Challenges, such as complexity and accuracy concerns for the different registration techniques including different imaging protocols have been improved over the past few years, but have not yet led to general clinical applicability. This review highlights the need for further work in the field of dental multimodality image fusion.
Future recommendations
To explore the accuracy and clinical application of MRI-CBCT image registration in the field of craniofacial and TMJ. This review suggests the following:
-
1)
Measure the accuracy of the MRI-CBCT mutual information algorithm using a gold standard tool independent of MRI or CBCT.
-
2)
Test the usefulness of the fused MRI-CBCT in evaluating the TMJ among practitioners with different levels of expertise.
-
3)
Explore objective tools to measure disc position or changes in relation to osseous structure using 3D volume rendering.
Conclusions
There are very limited studies of MRI-CT/CBCT registration, with data insufficient to reach a conclusion regarding its accuracy or clinical use in the temporomandibular joints.
Mutual information based registration seems a promising technique, and exploring its accuracy and applications for TMJ analysis would be worthwhile in larger studies.
References
Lunsford LD, editor. Modern Stereotactic Neurosurgery. Boston, MA: Martinus Nijhoff; 1998.
Taylor R, Mittelstadt B, Paul H, Hanson W, Kazanzides P, Zuhars J, et al. An image-directed robotic system for precise orthopaedic surgery. IEEE Trans Robot Automation. 1994;10(3):261–75.
Adler Jr JR, Murphy MJ, Chang SD, Hancock SL. Image-guided robotic radiosurgery. Neurosurgery. 1999;44(6):1299–306. discussion 1306–7.
Hofstetter R, Slomczykowski M, Sati M, Nolte LP. Fluoroscopy as an imaging means for computer-assisted surgical navigation. Comput Aided Surg. 1999;4(2):65–76.
Bjork A. Facial growth in man, studied with the aid of metallic implants. Acta Odontol Scand. 1955;13(1):9–34.
Gu Y, McNamara Jr JA. Cephalometric superimpositions. Angle Orthod. 2008;78(6):967–76.
Honda K, Larheim TA, Maruhashi K, Matsumoto K, Iwai K. Osseous abnormalities of the mandibular condyle: diagnostic reliability of cone beam computed tomography compared with helical computed tomography based on an autopsy material. Dentomaxillofac Radiol. 2006;35(3):152–7.
Hilgers ML, Scarfe WC, Scheetz JP, Farman AG. Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am J Orthod Dentofacial Orthop. 2005;128(6):803–11.
Alsufyani NA, Dietrich NH, Lagravère MO, Carey JP, Major PW. Cone beam computed tomography registration for 3-D airway analysis based on anatomic landmarks. Oral Surg, Oral Med, Oral Pathol Oral Radiol. 2014;118(3):371–83.
Lagravre MO, Secanell M, Major PW, Carey JP. Optimization analysis for plane orientation in 3-dimensional cephalometric analysis of serial cone-beam computerized tomography images. Oral Surg, Oral Med, Oral Pathol, Oral Radiol Endodontol. 2011;111(6):771–7.
Gkantidis N, Schauseil M, Pazera P, Zorkun B, Katsaros C, Ludwig B. Evaluation of 3-dimensional superimposition techniques on various skeletal structures of the head using surface models. PLoS One. 2015;10:2.
Cevidanes LH, Bailey LJ, Tucker Jr GR, Styner MA, Mol A, Phillips CL, et al. Superimposition of 3D cone-beam CT models of orthognathic surgery patients. Dentomaxillofac Radiol. 2005;34(6):369–75.
Cevidanes LH, Styner MA, Proffit WR. Image analysis and superimposition of 3-dimensional cone-beam computed tomography models. Am J Orthod Dentofacial Orthop. 2006;129(5):611–8.
Choi JH, Mah J. A new method for superimposition of CBCT volumes. J Clin Orthod. 2010;44(5):303–12.
Al-Saleh MA, Jaremko JL, Alsufyani N, Jibri Z, Lai H, Major PW. Assessing the reliability of MRI-CBCT image registration to visualize temporomandibular joints. Dentomaxillofac Radiol. 2015;44(6):20140244.
Nebbe B, Major PW, Prasad NG, Hatcher D. Quantitative assessment of temporomandibular joint disk status. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(5):598–607.
Pawiro SA, Markelj P, Pernus F, Gendrin C, Figl M, Weber C, et al. Validation for 2D/3D registration I: A new gold standard data set. Med Phys. 2011;38(3):1481–90.
Tai K, Park JH, Hayashi K, Yanagi Y, Asaumi JI, Iida S, et al. Preliminary study evaluating the accuracy of MRI images on CBCT images in the field of orthodontics. J Clin Pediatr Dent. 2011;36(2):211–8.
Dai J, Dong Y, Shen SG. Merging the computed tomography and magnetic resonance imaging images for the visualization of temporomandibular joint disk. J Craniofac Surg. 2012;23(6):e647–8.
Dai J, Wang X, Dong Y, Yu H, Yang D, Shen G. Two- and three-dimensional models for the visualization of jaw tumors based on CT-MRI image fusion. J Craniofac Surg. 2012;23(2):502–8.
Levitt MR, Vaidya SS, Su DK, Moe KS, Kim LJ, Sekhar LN, et al. The "triple-overlay" technique for percutaneous diagnosis and treatment of lesions of the head and neck: Combined three-dimensional guidance with magnetic resonance imaging, cone-beam computed tomography, and fluoroscopy. World Neurosurg. 2013;79(3–4):509–14.
Lin YL, Liu YH, Wang DM, Wang CT. Three-dimensional reconstruction of temporomandibular joint with CT and MRI medical image fusion technology. Hua Xi Kou Qiang Yi Xue Za Zhi. 2008;26(2):140–3.
van den Elsen P, Pol E, Viergever A. Medical image matching - a review with classification. Eng Med Biol Mag, IEEE. 1993;12(1):26–39.
Maintz JB, Viergever MA. A survey of medical image registration. Med Image Anal. 1998;2(1):1–36.
Wang X, Li L, Hu C, Qiu J, Xu Z, Feng Y. A comparative study of three CT and MRI registration algorithms in nasopharyngeal carcinoma. J Appl Clin Med Phys. 2009;10(2):2906.
Moore CS, Liney GP, Beavis AW. Quality assurance of registration of CT and MRI data sets for treatment planning of radiotherapy for head and neck cancers. J Appl Clin Med Phys. 2004;5(1):25–35.
Veninga T, Huisman H, van der Maazen RW, Huizenga H. Clinical validation of the normalized mutual information method for registration of CT and MR images in radiotherapy of brain tumors. J Appl Clin Med Phys. 2004;5(3):66–79.
West J, Fitzpatrick JM, Wang MY, Dawant BM, Maurer Jr CR, Kessler RM, et al. Comparison and evaluation of retrospective intermodality brain image registration techniques. J Comput Assist Tomogr. 1997;21(4):554–66.
Al-Saleh MA, Punithakumar K, Jaremko JL, Alsufyani NA, Boulanger P, Major PW. Accuracy of magnetic resonance imaging-cone beam computed tomography rigid registration of the head: an in-vitro study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016;121:316–21.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no competing interest.
Authors’ contribution
MA conceived of the study, prepared its design and coordination, acquisition of data, analysis and interpretation of the data and drafted the manuscript. NA and HS participated in the articles screening and scoring process and helped in drafting the manuscript. JJ and PM participated in drafting the manuscript and critically revised it for important intellectual content, and provided final approval of the version to be published. All authors read and approved the final manuscript for publication.
Additional file
Additional file 1:
Search strategy. (DOCX 22 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Al-Saleh, M.A.Q., Alsufyani, N., Saltaji, H. et al. MRI and CBCT image registration of temporomandibular joint: a systematic review. J of Otolaryngol - Head & Neck Surg 45, 30 (2016). https://doi.org/10.1186/s40463-016-0144-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40463-016-0144-4